
Navigating patient consent in the age of digital healthcare

As health data increasingly flows across applications, AI systems, insurers, hospitals, and wearable devices, consent plays an increasingly central role in governing how sensitive information is collected, shared, and accessed.
Because digital health services store and share data in ways that are rarely obvious to the patient, this exchange is far more abstract than traditional person-to-person care. To maintain trust, patients must have absolute clarity: exactly what information is being gathered, for what purpose it is used, where it is stored, and who is granted access.
The global challenge of health data
This framework should include the right of the individual to revoke their consent as easily as they provided it. However, this is one of many areas where consent implementation and interpretation become complex due to varying legal requirements across the globe.
The management of consent depends significantly on an individual’s location, the jurisdiction of their healthcare provider, and the specific institution handling their information. Adding to this complexity, what legally qualifies as 'health data' is not always straightforward.
This article explores the global tug-of-war between privacy and technology, specifically the EU vs US models, and outlines the essential functionalities a modern Consent Management Platform (CMP) must provide to navigate this complex landscape.
Regulation landscape
The EU & UK model: Privacy by design and data sovereignty
The GDPR serves as the foundational pillar for data protection across both the EU and the UK. While they are now separate legal frameworks (the EU GDPR and the UK GDPR) they remain closely aligned in their core principles, and act as the primary regulations for managing patient consent. On top of this shared foundation, each region layers its own specific health regulations that provide extra protections or specific instructions for how sensitive medical data must be handled in practice.
The right to revoke consent is absolute and legally mandated under the GDPR. Withdrawing consent must be as easy as giving it and it halts all active data processing immediately. Right to erasure (Right to be forgotten) is in most cases exercised as a follow-up; this means the provider must delete your data unless they have a specific legal reason to keep it (such as a tax record, a medical safety log, or a public health requirement).
EU-Specific Frameworks: EHDS and AI Governance
The European Health Data Space (EHDS) mandates that health apps be "interoperable" and grants patients a specific "opt-out" right regarding the use of their data for research. For clinical studies, the Clinical Trials Regulation (CTR) is applied, requiring a strictly regulated Informed Consent process to ensure participants understand every risk before a single data point is collected.
Complementing these is the EU AI Act, which classifies most health-related AI as “high risk,” imposing extra transparency requirements on how the AI is trained and how data is utilised.
UK-Specific Frameworks: Confidentiality and the 2025 Act
The UK employs a unique "Double Lock" to protect patient information – it requires providers to satisfy both technical UK GDPR standards and the long-standing ethical Common Law Duty of Confidentiality.
Within the NHS system, the National Data Opt-Out policy allows patients to consent to the use of their data for their own care and to refuse consent for its use in research or planning. Most recently, the UK updated its framework with the Data (Use and Access) Act 2025, making it slightly easier for scientific research to access data. To balance this, the Act has also introduced a right to complain that enforces a strict 30-day response deadline for any institution mishandling data.
EU AI Act in healthcare: Beyond compliance to strategic resilience
The EU AI Act isn't just a compliance hurdle; it’s redefining clinical-grade AI. With strict deadlines approaching, retrofitting systems is costly. Learn how to classify your AI portfolio, design for transparency, and turn regulatory requirements into a strategic advantage.
Learn moreThe US Model: Interoperability, clinical flow, and TPO
Sectoral Division and HIPAA
One of the specifics of the US regulation landscape is the “sectoral division”, meaning there is no single, overarching federal law like the GDPR. Instead, your privacy rights depend entirely on who holds your data.
HIPAA remains the primary federal law, but it applies only to "covered entities", specifically doctors, hospitals, and health insurers. If you use a fitness app or a smart device that is not directly connected to your healthcare provider, your data is likely not covered by HIPAA.
TPO consents and the limits of revocation
Unlike the GDPR, HIPAA permits data sharing for Treatment, Payment, and Operations (TPO) without specific consent. Patients don't "opt-in"; they simply acknowledge a Notice of Privacy Practices (NPP), allowing their data to flow automatically between doctors and billing departments.
A specific authorisation is only required for "extra" activities, such as marketing or sharing data with a life insurance company.
Another major distinction between the EU and the US landscape is how the revocation of consent is handled. One can revoke that authorisation in writing at any time, but the effect is purely prospective, meaning it typically only applies to the future. Anything the company already shared or did with their data while the consent was active remains legally valid and cannot be retracted.
The Right to be Forgotten also functions differently in the US. American medical providers are required by state and federal laws to retain your records for significant periods (often 6 to 10 years, and sometimes much longer for minors). You can't just tell a hospital to "delete everything", as you might with a consumer tech company in Europe, because these retention mandates overrule the individual’s request for erasure.
Wearables and the non-HIPAA blind spot
As mentioned above, the data handled by wearables and health trackers is usually not under the jurisdiction of HIPAA. In these cases, the Federal Trade Commission (FTC) acts as the primary enforcer of privacy promises, and a growing patchwork of state-specific regulations creates a regulatory network that can be a tough labyrinth to navigate.
To bridge this gap, there are ongoing legislative proposals to force "non-HIPAA" entities to follow the same strict consent and security standards as hospitals, like the Health Information Privacy Reform Act.
Consent basics
The mechanics of consent: Opt-in/out and explicit/implicit
Before examining the technologies that manage consent, let us first explain the distinction between the primary modes of consent used in modern healthcare: opt-in and opt-out. These define the default state of interaction between a system and an individual.
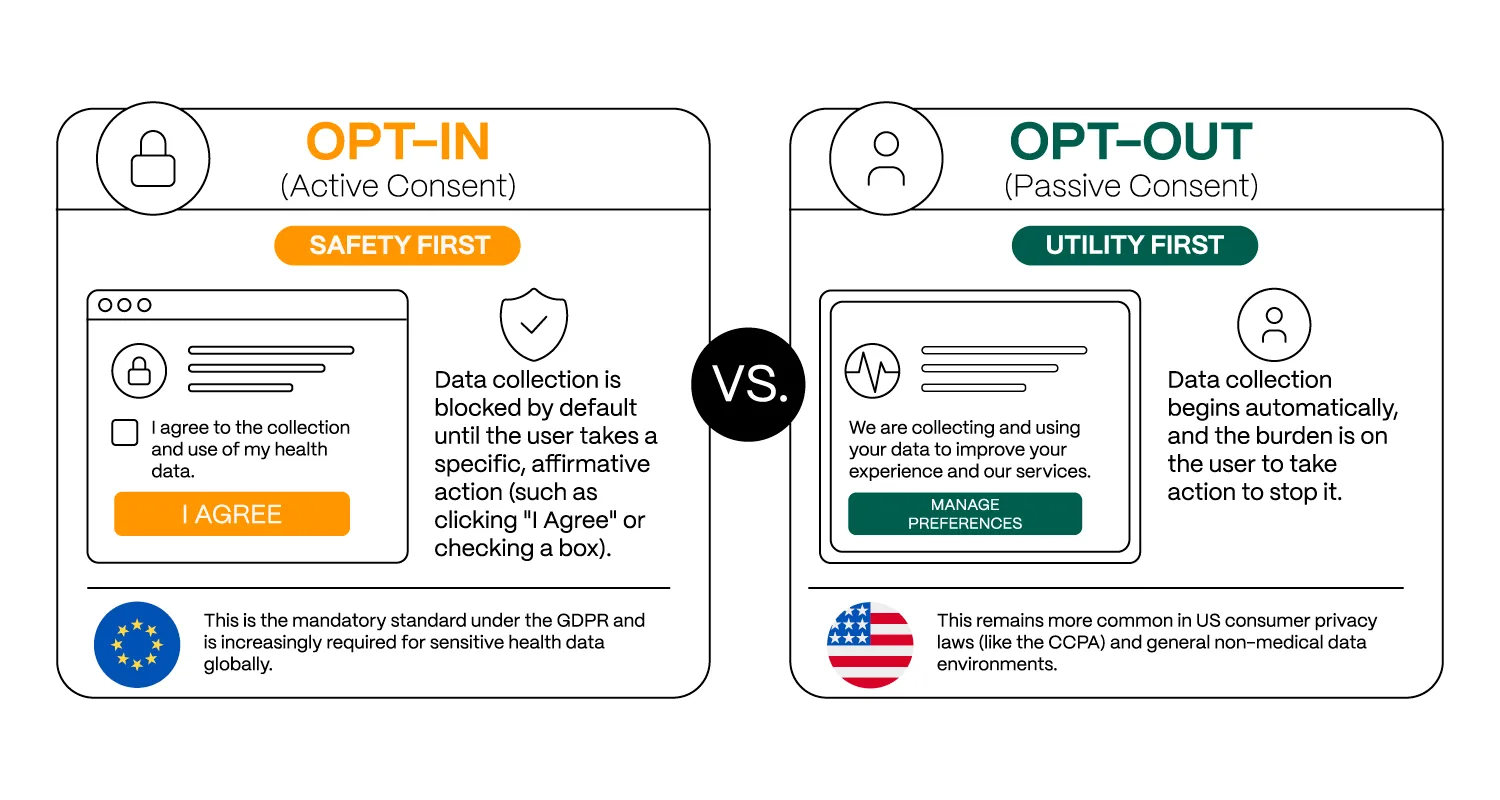
- Opt-In (Active Consent) follows a “safety-first” model in which data collection is blocked by default until the user provides explicit affirmative action, such as selecting “I agree” or checking a consent box. This approach is mandated under GDPR for many categories of sensitive data and is widely applied in healthcare contexts.
- Opt-Out (Passive Consent) follows a “utility-first” model in which data collection is enabled by default, while users retain the ability to withdraw permission afterward. This model remains more common in non-medical or consumer-oriented regulatory environments.
A further distinction exists between explicit and implicit consent. While these concepts are often treated as synonymous with opt-in and opt-out, there is a subtle distinction: one set explains how you give permission (the action), while the other defines the system's default state (the rule).
- Explicit consent requires a deliberate affirmative action, such as signing a form, clicking a button, or selecting a permission option.
- Implicit consent, by contrast, is inferred from the patient’s actions or the context of the situation. In telemedicine platforms, a patient joining a scheduled video consultation may implicitly permit the clinician to access the records necessary for the appointment.
Beyond the mechanism of agreement, healthcare systems must also account for Informed Consent, particularly in clinical research. In this context, it is not enough to simply get a 'Yes’ from a participant. The researcher must prove the individual understood the scope, risks, and implications of participation. In 2026, informed consent has evolved into a structured and regulated electronic process.
From snapshots to living dialogues: Static vs dynamic consent
Historically, systems relied on static consent – inflexible "snapshots" captured in paper forms, PDFs or database entries. Today, Dynamic Consent is the gold standard. Managed through secure digital portals, it acts as a "living" agreement, allowing patients to update or revoke their preferences in real time.
Defining scope and depth: Specific, broad, and tiered consent
Consent in healthcare rarely operates as a single binary choice. Instead, it varies in scope and granularity.
- Specific Consent limits data use to a single, narrowly defined purpose (e.g., a single beta blocker study). This approach is strongly privacy-oriented, but it can slow down research progress by requiring researchers to repeatedly obtain permission for each new project. Managing many individual-specific consents can become burdensome for both systems and participants.
- Broad Consent allows data to be used within a predefined domain, such as cardiovascular research conducted within a particular institution. This model is widely used in biobanking and longitudinal population health studies.
A modern system must also manage the depth of this data through Tiered Consent. Rather than treating all health information as a single block, this approach categorises data by sensitivity:
- Core Tier: Data essential for direct care and operations.
- Research Tier: De-identified or pseudonymised data used for scientific analysis.
- High-Sensitivity Tier: Highly protected data such as genetic information, reproductive health records, or mental health documentation.
As is usually the case, different modes serve different purposes and often coexist within a single system. For example, a broad consent might be granted for general research across a core tier of data, while a specific, restricted lock is maintained for a patient’s high-sensitivity tiers of information.
From models to implementation: Standards for machine-readable consent
These conceptual models increasingly require formal, machine-readable representations within digital health systems. As a result, modern HealthTech architectures are transitioning from document-centric approaches such as IHE BPPC (Basic Patient Privacy Consents) toward more structured and computable frameworks, including IHE APPC (Advanced Patient Privacy Consents) and the HL7 FHIR Consent resource.
These standards make it possible to express consent rules in a structured form that can be evaluated by external authorisation systems. As a result, healthcare systems can make access decisions based on attributes such as data type, user role, and purpose of use, even when data is shared across distributed environments.
Consent Management Platforms (CMPs)
Navigating this layered complexity, while automating the collection and enforcement of user preferences, has driven the adoption of dedicated Consent Management Platforms (CMPs) tailored for healthcare.
Typically, a CMP manages the entire lifecycle of a patient's choice: from presenting a user interface with opt-in/opt-out notices, to creating time-stamped records of an individual’s decisions, to providing a robust audit trail. Most importantly, they serve as orchestrators of data-gathering components, ensuring that health data only flows when proper digital consent is in place.
Smart and granular control
A true healthcare CMP must manage data sensitivity levels, as not all health information is treated equally. For instance, information such as mental health notes or HIV status often requires stricter legal protections than a simple step count. In such cases, the CMP acts as a smart filter. It applies specific rules based on data type and the user’s local laws, ensuring that even within a single app, different “buckets” of data are governed by different sets of digital permissions.
Modern platforms must support granular and dynamic control. This means that a patient can say “yes” to their data being used for direct care by their doctor but say “no” to secondary uses such as marketing or AI training. Instead of a one-time paper form, the patient has a portal where they can change their mind in real time.
FHIR standards: The "remote control" for patient data
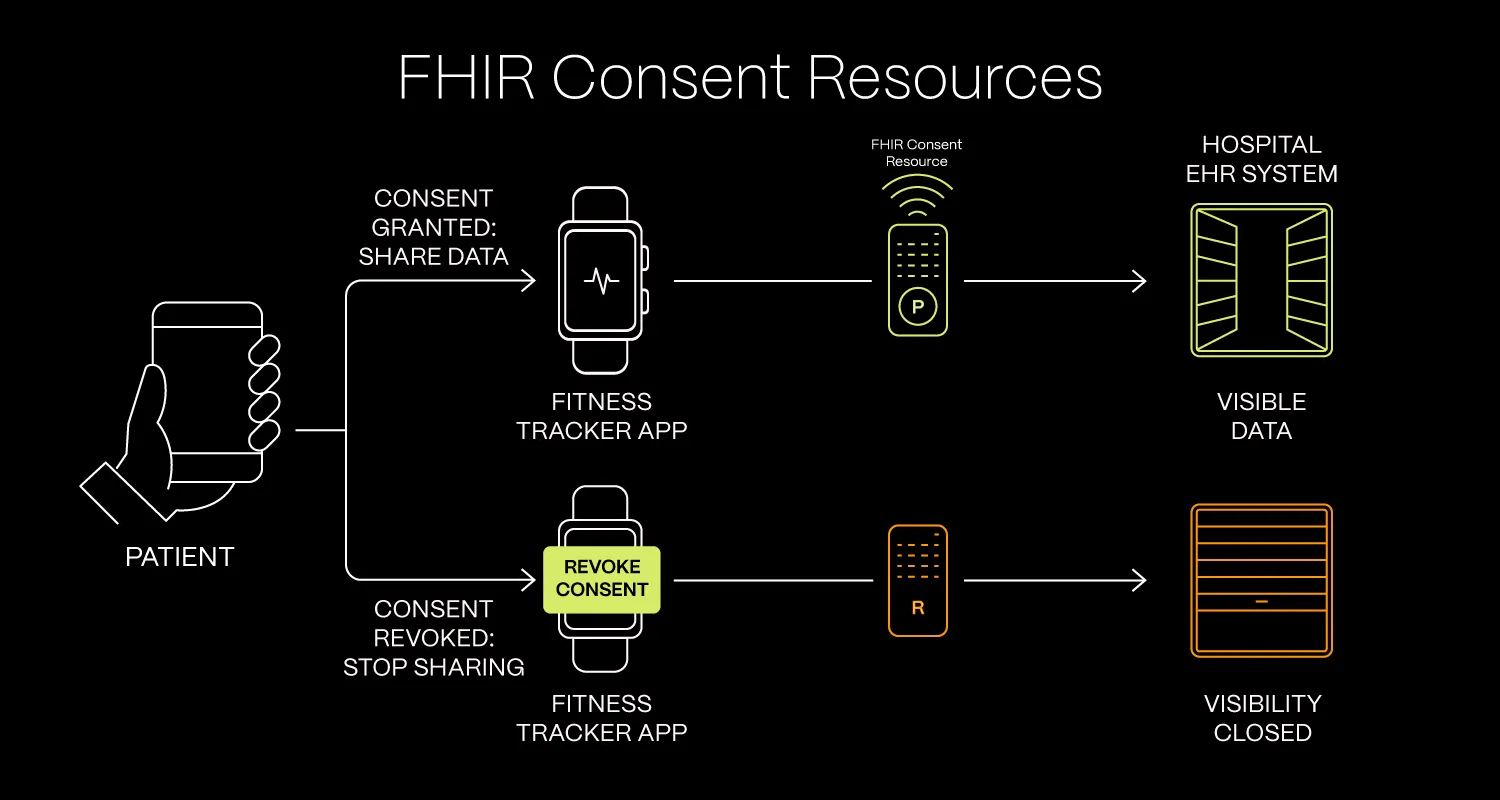
One of the basic functionalities a true CMP has to deliver is interoperability between apps, hospitals, and pharmacies. In practice, this means modern CMPs are expected to support the communication of the FHIR Consent Resource across all platforms handling an individual’s data. You can think of this resource as a "remote control" for patient data. It travels with the information and dictates which data points can be used, for what specific purpose, and by which authorised service.
For example, if a patient authorises data sharing between a fitness tracker application and a hospital Electronic Health Record (EHR) that permission can be encoded as a FHIR Consent Resource and transmitted to the healthcare institution’s system. If the patient later revokes consent within the application, the updated consent status may likewise be communicated back through FHIR-based interoperability workflows, allowing the receiving system to apply updated access-control policies.
In practice, the consent signal functions like a “digital shutter”: although the data may remain stored within the system for legal, regulatory, or auditing purposes, updated access-control policies can effectively “close” visibility to unauthorised users or services.
Handling emergencies: "Break-Glass" provisions
"Break-glass" provisions are a critical feature in healthcare systems. In life-threatening situations, clinicians may be permitted to override standard access restrictions to retrieve necessary patient data. Naturally, such access is subject to strict governance and is accompanied by comprehensive audit logging, capturing who accessed the data, when it was accessed, which records were involved, and the justification for the emergency use.
Finally, a CMP should support multi-party and delegated consent, recognising the vital role of caregivers and legal guardians in the decision-making process.
The future of consent: Trust as infrastructure
Navigating the HealthTech consent landscape requires a multidisciplinary understanding of evolving legislation, data sensitivity, and technical interoperability. To uphold the ethical and privacy principles central to healthcare, modern systems must treat consent as a dynamic and continuously evolving process.
Addressing this complexity is essential for building digital healthcare solutions that protect patient autonomy while supporting ongoing innovation in medical practice.
